
Trends Report

Momentum in a Complex Era
Scalable AI, accelerated access to care, and evidence-driven insight guiding the path forward
Our world, and industry, are increasingly defined by disruption, volatility, and rising complexity. Aging workforces, growing comorbidities, and higher financial exposure are reshaping the profile of the modern claim. Operational efficiency alone is no longer sufficient. And yet, beneath the surface, there are meaningful signs of progress. The industry is not standing still. In several critical areas, it is moving forward.
This year’s report highlights three forces driving that momentum:
PART 1
PART 2
Looking across multiple injuries and treatment pathways, one signal stands out. The industry’s pipeline to care is improving, with injured individuals reaching appropriate treatment more efficiently.
To illustrate how this shift affects recovery, we examine two services that shape the early course of a claim: conservative care and advanced imaging.
PART 3
Recent research reinforces a consistent theme: early insight, appropriate utilization, and thoughtful intervention meaningfully influence recovery and total claim trajectory.
When AI-driven intelligence is paired with a more efficient care pathway and grounded in current clinical research, the result is a framework capable of managing complexity with greater confidence and optimism.
PART 1
AI Adoption in Workers’ Comp & Auto Casualty: From Hype to Operational Advantage
For claims organizations navigating rising severity and growing complexity, the window to build durable AI capability is now.
AI Is Now a Core Capability
AI is no longer a side project in healthcare or casualty claims.
It is becoming part of the operating system for payers, TPAs, and the partners they rely on. The real shift is in the need to decide where AI belongs in the workflow and how it changes claim economics. For workers’ comp and auto casualty, the environment is shifting: claim frequency continues to decline while severity trends higher, and claims organizations are still managing meaningful operational burden from administrative workload and fragmented systems.
Pilot Purgatory Creates Real Costs
Across industries, organizations have moved from asking whether to adopt AI to figuring out how to scale it responsibly.
In insurance and claims specifically, executive priority is high, but scaled production remains the bottleneck. That is the gap that matters for payers: a flood of pilots and point tools does not automatically translate into cycle time reduction, better recovery, or lower total cost. Many programs stall because of the hard work required up front in integration: clean data, governance, and workflow ownership that turns AI from a demo into measurable operational advantage.
In many claims organizations, AI changes the shape of work before it changes the cost of work. There is risk in adopting AI too slowly, and there is risk in adopting it in ways that increase friction, noise, and variability at exactly the moment claims leaders need predictability and throughput. Without workflow redesign, it can shift effort into review, oversight, exception handling, and rework, creating even more operational friction.
The Claim Mix is Growing More Complex
The urgency is not theoretical.
Claim frequency may be trending down, but the claims that remain are becoming harder to resolve quickly and cleanly. In workers’ comp, the share of injured workers aged 50+ has increased, and comorbidities have risen over time. Both can slow recovery and increase the likelihood of complications, extended utilization, and disputes. At the same time, low-severity cases are shrinking as a share of the mix, which means the average claim carries more complexity and more financial exposure. Better decisions earlier in the claim matter more than ever, and the organizations that can reliably identify risk and remove friction will win.
Foundation First Creates Operational Advantage
So what separates success from backfire? Readiness.
The organizations getting durable results treat AI as an operating model change, not a technology add-on. That starts with data that is longitudinal, governed, and usable in real workflows. It continues with clear controls on how AI is applied, where humans make final decisions, and how outcomes are measured over time. It also requires designing for the realities of regulated healthcare and casualty claims: transparency, auditability, and a phased approach that earns trust while steadily expanding impact. When those foundations are in place, AI can compress cycle times and reduce unnecessary spend without creating new risk.
For workers’ comp and auto casualty payers, the goal is to translate AI into outcomes that matter: faster recovery, less medical variability, fewer downstream disputes, and smarter total cost management. That means prioritizing adoption where it removes friction and improves decision quality across the claim journey, not simply where it looks impressive in isolation. The next chapter of competitive advantage will belong to the organizations that operationalize AI responsibly, at scale, and in service of better recovery and better economics.
PART 2
Collective Success: Improving the Pipeline to Care
Despite rising claim complexity, patients are entering treatment sooner across a wide range of injury categories. Here’s what the data shows and what it signals for the industry.
The Pattern is Clear and it’s Getting Stronger
Across our bill review and physical therapy data, a clear pattern has emerged over the past 5 years. Despite an increase in claim complexity, patients are entering treatment sooner across a wide range of injury categories.
We describe this as improvement in the “pipeline to care,” the full process from injury through referral, authorization, and initiation of treatment. Our data indicates:

The pipeline to care process is functioning more efficiently than in prior years
Time to treatment is decreasing
Care delivery is becoming more consistent across providers and markets.
Notably, this pattern is not isolated to one diagnosis or treatment pathway. The movement appears across multiple injury types, suggesting broader process improvement rather than isolated changes in clinical behavior.
These improvements reflect how the system is operating. Enhancements in documentation, referral coordination, peer review efficiency, and claims processing all appear to be contributing. The signal is operational as much as clinical, pointing to a system that is moving patients into appropriate care with less friction.
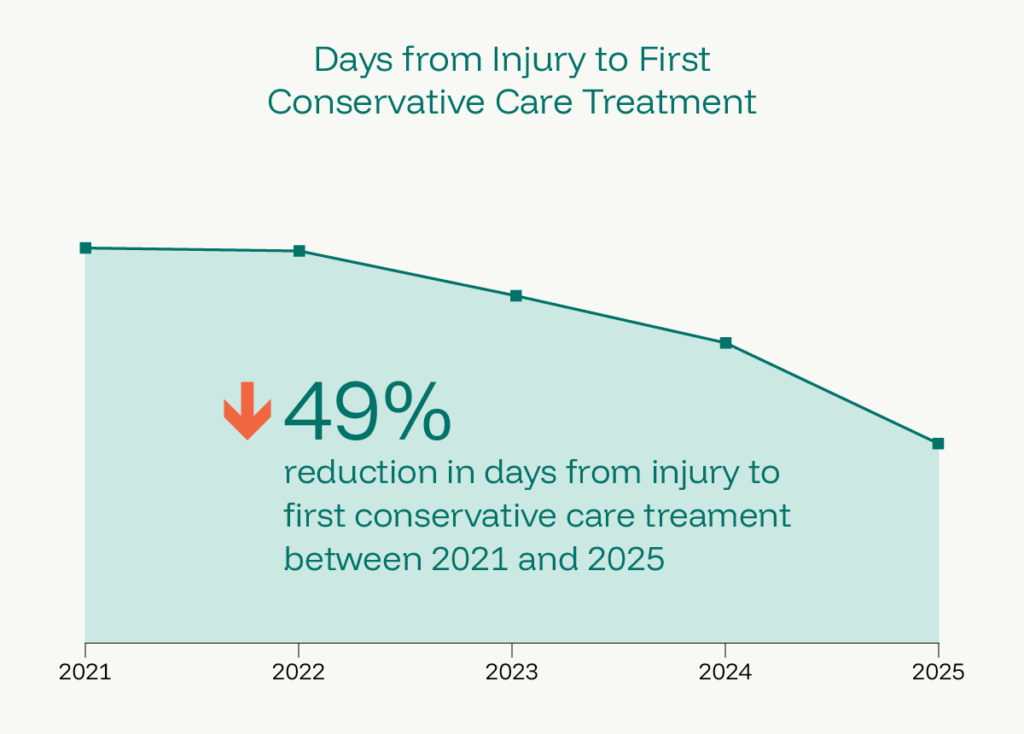
Days from injury to first conservative treatment for non-radicular lumbar spine pain decreased 50% between 2021 and 2025. This trend of patients beginning conservative treatment sooner than in previous years is seen consistently across ICD groups.
Earlier Access to Conservative Care
One of the most significant developments is faster entry into conservative treatment, particularly physical therapy. Our data shows that patients are beginning conservative treatment sooner than in previous years, and that access is becoming more uniform across the industry.
Delays in initiating therapy have historically been associated with prolonged disability, greater reliance on pharmaceuticals, and higher rates of advanced interventions. Moving patients into appropriate conservative treatment earlier in the life of a claim supports better functional recovery and more stable downstream outcomes.
Importantly, this trend does not suggest that care is being rushed. Rather, we infer that it reflects improvements in efficiency throughout the system of care that have reduced administrative and logistical barriers to evidence-based first line treatment.
Advanced Imaging: Deliberate and More Efficient
A similar pattern is visible in advanced imaging, specifically MRI and CT. This does not reflect an increase in imaging orders overall, or a loosening of clinical criteria.
What it reflects is that patients who meet the threshold for advanced imaging are having those studies completed more rapidly and earlier in the course of treatment. When imaging is clinically appropriate, faster access can help set patients on a more timely treatment trajectory.
Imaging utilization has long been variable across the industry. Some providers take an expansive approach, while others follow a more selective, guideline-driven model. The broader trend does not signal indiscriminate imaging. It points to improved workflow and clearer clinical decision-making.

Days from injury to advanced imaging shows more efficient navigation of clinical criteria and authorization processes.
The trends observed in this data reflect a treatment pipeline that has adapted to administrative and social factors in the post-COVID era. The favorable decrease in time to treatment of any sort shown by our data are likely multifactorial. Each industry entity should remain mindful of the needs of patients as we work toward providing outcomes with minimal impairment and no long-term disability. These data reflect the sum of the internal process a patient experiences from the date of injury to treatment milestones such as imaging, PT or surgery.
Balancing Speed and Utilization
Faster access to care is a meaningful improvement, but speed alone is not the goal. At the same time, overutilization remains a meaningful risk, particularly in areas such as advanced imaging. The industry continues to balance two important priorities: reducing unnecessary delay and maintaining disciplined, evidence-based utilization management.
The data suggests that this balance is improving. Patients are entering conservative care sooner, and advanced imaging appears to be occurring more efficiently within established criteria. The broader signal is not one of excess, but of better alignment between clinical judgment and administrative processes.
Maintaining that balance will remain critical. Efficiency should support appropriate care, not substitute for it.
We encourage readers to compare their own internal practices and performance to the industry median. Outliers may reflect target areas for process improvement. Faster treatment, reflecting an easier process for patients and treatment providers, is strongly associated with the most favorable recovery outcomes.
What This Signals for the Industry
Taken together, these trends point to a maturing operational environment.
The improvements appear to reflect better coordination among stakeholders, clearer documentation standards, more streamlined referral pathways, and more consistent authorization processes. Rather than being driven by changes in injury severity or diagnosis mix, the shift appears rooted in how the system functions.
A more efficient pipeline to care reduces friction at critical early decision points in a claim. When patients enter appropriate conservative treatment sooner and necessary diagnostics occur without unnecessary delay, the trajectory of recovery can be positively influenced.
Operational discipline and clinical alignment are increasingly working in tandem.
As the industry continues to refine processes and maintain thoughtful utilization oversight, earlier and more consistent access to appropriate care may become the standard rather than the exception.
PART 3
Clinical Evidence that Moves the Needle
Recent research reinforces three areas where the evidence is moving fast and implications for claims management are clear.
RTW & Recovery
New evidence on how opioid use before spine surgery cuts return-to-work odds in half; why early physical therapy and biopsychosocial care outperform early opioids; what drives RTW timelines; and how workplace social support determines whether recovery sticks.
Utilization & Cost
How patterns of early service use predict downstream disability and spend; why opioid prescribing in the first weeks after injury has outsized effects on both return-to-work rates and workers’ compensation expenditures.
Policy & System design
What happens to workers after claims close and why it’s often not what the file suggests; global perspectives on access, liability, and equity in WC systems; and why provider training in navigating return to work is underutilized and undervalued.
Wide Variation in Lumbar Spine Fusion Decisions
79% of injured workers successfully returned to work after treatment for work-related injuries
Clinical Summary
Among spine surgeons treating similar lumbar conditions, use of instrumented fusion ranged from 0% to over 90%. These differences were associated with meaningful variation in major in-hospital complications and 30-day readmissions. Training and higher operative volume were linked to lower complication rates.
What It Means for Casualty Claims
The same diagnosis can lead to very different surgeries depending on the surgeon. When fusion rates vary from almost never to almost always, claim outcomes will vary too. Referral strategy and surgeon performance matter because surgical choice directly affects recovery time, complication risk, and total spend.
MRI Abnormalities Are Nearly Universal in Adult Shoulders
99% of adults aged 41–76 had rotator cuff abnormalities on MRI — including those with no pain.
Clinical Summary
In adults aged 41 to 76, 99% had at least one rotator cuff abnormality on MRI. Abnormalities were present in 96% of asymptomatic shoulders and 98% of symptomatic shoulders, showing minimal difference between those with and without pain.
What It Means for Casualty Claims
When nearly everyone shows “abnormal” findings, imaging alone cannot define the problem. If structural changes are treated as the cause of pain without clinical context, care can escalate unnecessarily. Functional assessment should guide decisions, not the MRI report alone.
Joint Replacement Surgeries Are Rising in Workers’ Compensation
$116K–$129K average total medical cost · 43–55 weeks average disability duration
Clinical Summary
Rates of major joint replacement surgeries per 1,000 lost-time claims have increased over time. These claims often exceed $116,000 to $129,000 in total medical costs and are associated with temporary disability durations of roughly 43 to 55 weeks.
What It Means for Casualty Claims
Joint replacements represent some of the highest-cost, longest-duration claims in the system. As utilization grows, ensuring appropriate patient selection and strong conservative pathways becomes essential to managing both recovery and portfolio risk.
Most Workers Return to Work After Injury
$116K–$129K average total medical cost · 43–55 weeks average disability duration
Clinical Summary
Across studies, 79% of injured workers successfully returned to work. However, outcomes varied based on factors such as age, education level, and injury type.
What It Means for Casualty Claims
The majority of workers do get back to work, which is encouraging. The opportunity lies in identifying the roughly 1 in 5 who may struggle and intervening early with targeted support before disability becomes prolonged.
Preoperative Opioid Use Predicts Poorer Surgical Recovery
Preoperative opioid users had ~half the odds of stable return to work after spinal surgery.
Clinical Summary
Workers’ compensation patients using opioids before spinal surgery had about half the odds of achieving stable return to work compared to non-users.
What It Means for Casualty Claims
Cutting return-to-work odds in half is not a small signal. Preoperative opioid use is a clear risk indicator for extended disability. Early pharmacy oversight and behavioral risk management can materially influence surgical outcomes and claim duration.
Claim Closure Does Not Equal Full Recovery
A systematic scoping review found that injured workers are generally disadvantaged in some manner following claim finalization
Clinical Summary
Research consistently shows that many injured workers experience ongoing financial, vocational, and psychosocial challenges even after their workers’ compensation claim is finalized.
What It Means for Casualty Claims
Administrative resolution does not always equal durable recovery. If recovery stability is not supported at transition, downstream risks such as re-entry, dissatisfaction, or litigation may follow. Long-term outcomes matter beyond the claim file.
THE CONSISTENT THEME
What the Evidence Tells Us
Across these six studies, one pattern holds: the decisions made early in a claim, such as who treats the patient, how imaging is interpreted, what the medication history reveals, and when conservative care begins shape everything that follows. The evidence does not point to radical change. It points to disciplined execution of what works.
Early insight. Appropriate utilization. Thoughtful intervention. When those three things operate together, recovery improves and total claim trajectory stabilizes.
The Experience Behind the Analysis
MedRisk, with SPNet, Medata, StrataCare, and HCS Network Solutions is dedicated to lowering costs and accelerating recovery for injured workers in the casualty claims industry. As medical costs rise, MedRisk addresses these challenges with innovative managed care, payment integrity, and network solutions powered by data, AI, and analytics. Through care direction, care engagement, payment integrity solutions, networks and negotiations, payment solutions, and insights management, we ensure high-quality, timely care—enabling faster, seamless recoveries for patients and reducing administrative burden for adjusters and case managers. Here’s a closer look at MedRisk based on 2025 data:
