
Trends Report

MedRisk has always been dedicated to understanding and advancing best practices.
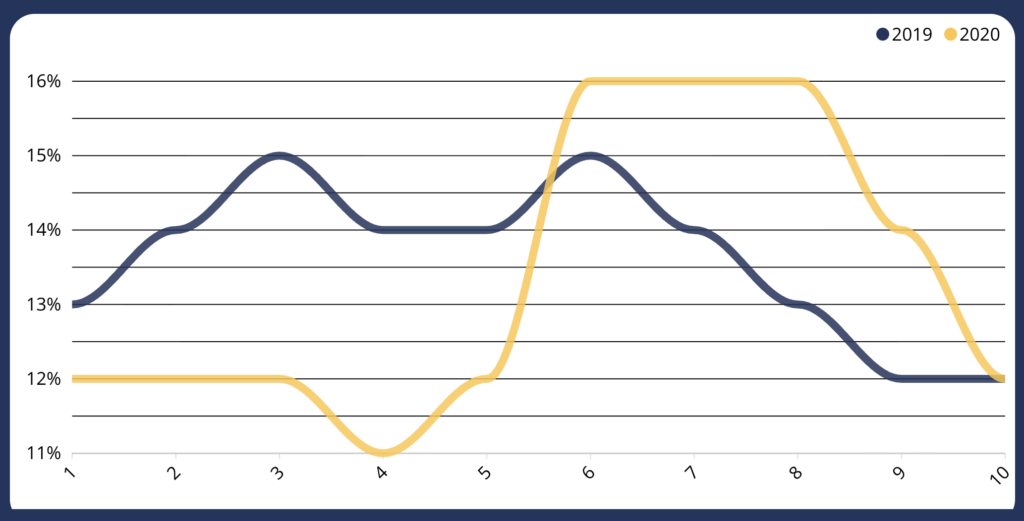
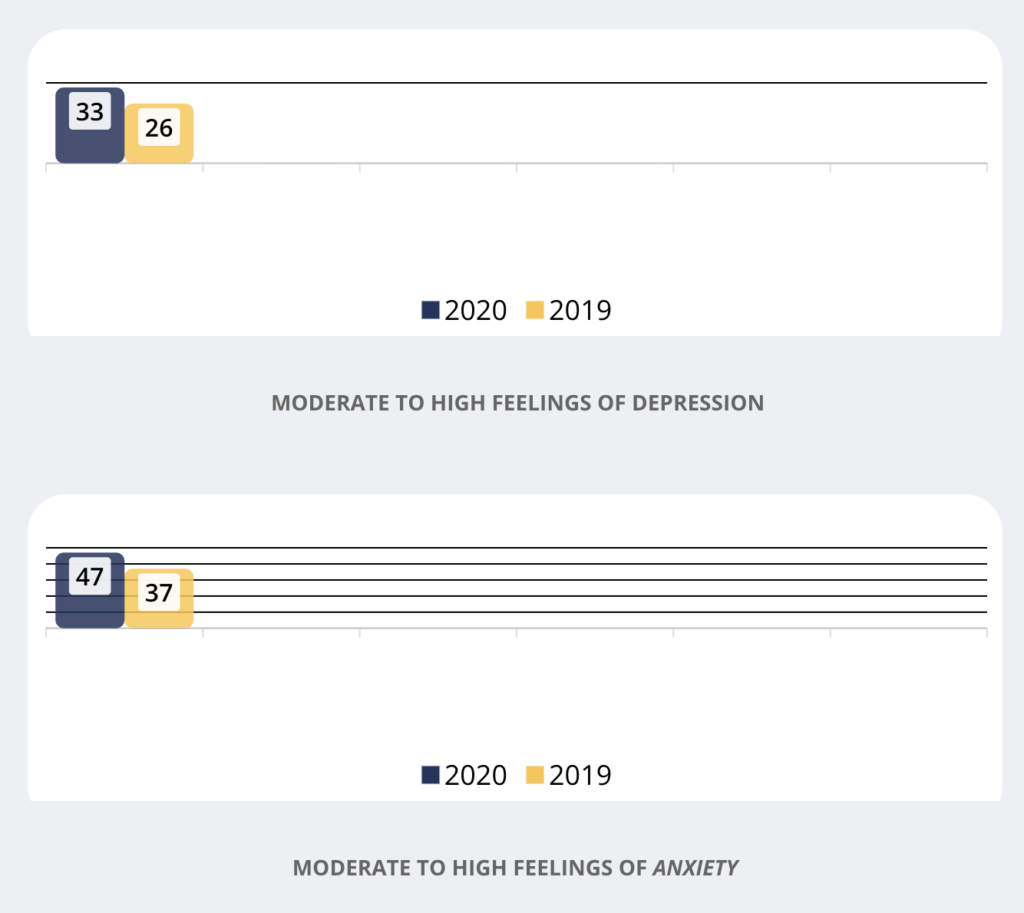
The Impact of COVID-19
Key Trends
45
40%
123%
Trending at MedRisk
Psychosocial Barriers to Recovery
Legislative Recap
The Department of Workers’ Claims has proposed Administrative Regulation 803 KAR 25:260, which adopts the ODG treatment guidelines broadly applied to non-emergency medical care. Treatment recommended in the guidelines would be presumed to be reasonable and necessary. Conversely, treatment not recommended or not addressed in the guidelines would require preauthorization, with the burden placed on the provider to justify the proposed treatment. For retrospective bills, payers would not be responsible for paying for treatment outside the guidelines unless it (a) was provided in a medical emergency, (b) was authorized by the payer, or (c) was approved via dispute resolution by an administrative law judge.
Implications: Once formally adopted, the new Administrative Regulation will add Kentucky to the list of jurisdictions that use independently developed interstate medical treatment guidelines to promote effective medical care while reducing friction within the WC system. The treatment guidelines apply to all treatment administered on and after September 1, 2020.
Senate Bill 381 adds a new section to the existing statute (NRS 616B.527) permitting payers to contract with preferred provider networks and giving payers the right to require injured workers to obtain healthcare services (including physical therapy) within the preferred provider organization. The new law imposes a qualification on employers’ and insurers’ ability to direct care: the injured worker must choose from the employer’s/insurer’s list of physicians and chiropractors only if the employer/insurer maintains a list of 12 physicians for each of the enumerated physician specialties and for 12 chiropractors.
The new law requires employers and insurers to maintain a list of physicians and chiropractors only, but not a list of PTs. If the payer doesn’t provide a list that complies with this requirement, the injured worker can select a physician or chiropractor from an approved list compiled by the WC Section of the Division of Industrial Relations. Further, the new law requires employers and insurers to file with the DIR an updated list of physicians and chiropractors by October 1 of each year.
Implications: The statute considerably restricts what has been a permissive approach to employer direction of care by imposing a “panel” requirement for physician specialties and chiropractors.P
The New York State Workers’ Compensation Board adopted several amendments to its regulations to conform them to the Expanded Provider Law taking effect on January 1, 2020. The amendments to the regulations implement the statute by detailing the billing process to be followed by newly authorized providers. The amendments clarify the regulations in three ways. First, the amendments provide that payers subject to the regulations include third party administrators as well as employers and insurers.
Second, the amendments add as new provider types protected by the regulation any authorized medical provider of Medical Care (defined broadly in the underlying statute to include physical and occupational therapists and acupuncturists, among others). Third, the amendments simplify the billing dispute process to eliminate the “continuous course of treatment” concept and to extend time to submit bills from 90 days to 120 days from the date of service. The amendments have an effective date of January 1, 2020.
Implications: The proposed amendments primarily conform the current regulations to the new statute and bolster the WCB’s enforcement powers over all payers, including TPAs. Lengthening the permitted provider bill submission timeline from 90 to 120 days after date of service, however, may necessitate changes to payers’ late-bill denial processes. The amendments retain their status as proposed rather than final, but payers may be well-served to comply with the proposed amendments sooner rather than later.
Research & Insights

Scaling Expertise in a Constrained Claims Workforce
The conversation around AI in workers’ compensation has covered familiar ground: staffing shortages, rising caseloads, and pressure on adjusters. These

The Value of Payment Integrity in Workers’ Comp
In workers’ comp, not all savings are created equal. Reimbursement strategies must be evaluated not just on low-cost unit price, but how they impact overall

MedRisk Supports Kids’ Chance of America at National Conference
Kids’ Chance’s purpose is simple: give kids of workers who have been injured on the job a chance at a

Clinical Evidence that Moves the Needle
Recent research reinforces three areas where implications for claims management are clear. RTW & Recovery New evidence on how opioid

MedRisk Acquires Horizon Casualty Services PPO Network Business
Strengthens MedRisk’s ability to deliver better outcomes and an elevated experience WEST CONSHOHOCKEN, Pa. — February 2, 2026 — MedRisk, a leading provider of

The World Shifted. So Did We.
The last few years reshaped everything. Not just how we work, but what’s possible. New Technology New Data New Expectations
MedRisk by the Numbers
90%
DECREASE IN TEMPORARY DISABILITY WITH EARLY PT VS LATE POST-INJURY PT
97.7%
OF NETWORK PROVIDERS AGREE WITH MEDRISK CLINICAL RECOMMENDATIONS
98.1%
PATIENT SATISFACTION
0
LAY-OFFS OR FURLOUGHS DURING COVID-19 SHUT DOWN
4
HOURS TO SCHEDULING
2.6
DAYS TO INITIAL EVALUATION
191,273
TOTAL NETWORK PROVIDERS
394,435
INJURED WORKERS TREATED